Abstract
This article traces a recurring pattern in United States addiction history: the repeated hope that one drug, regulation, or medical innovation could solve the harms produced by another. The Civil War helped create the nation’s first large-scale opioid crisis when morphine and opium were widely used to treat battlefield injuries, amputations, chronic pain, diarrhea, and lingering illness. In the late nineteenth century, Bayer marketed heroin as a safer, less addictive substitute for morphine, only for heroin itself to become recognized as highly addictive. The Harrison Narcotics Tax Act of 1914 then transformed narcotic control by requiring registration and taxation of those handling opiates and cocaine, while narrowing the space for maintenance prescribing. In the mid-twentieth century, methadone emerged as a more evidence-based response to heroin dependence. Today, medications for opioid use disorder save lives, but public skepticism persists because pharmaceutical marketing helped fuel the modern opioid epidemic. The article argues that effective addiction policy must move beyond a purely pharmacologic response and pair medications with long-term recovery supports, housing, social reintegration, and ethical regulation of industry influence.
Introduction
American addiction history can be read as a cycle of pain, relief, dependency, reform, and substitution. Throughout that history, the United States has repeatedly turned to chemical remedies to address the harms caused by earlier ones. At times, these substitutions were grounded in medical optimism; at other times, they were amplified by commercial interests and weak regulation. Understanding that pattern is essential for anyone writing about opioid use, treatment, and recovery today.
This pattern is especially visible in five moments: the morphine dependence that spread among Civil War veterans; Bayer’s marketing of heroin as a safer alternative to morphine; the Harrison Narcotics Tax Act’s turn toward federal control; the introduction of methadone maintenance for heroin addiction; and the contemporary debate over whether medications for opioid use disorder represent treatment, substitution, or both. When placed in sequence, these developments reveal that the central American struggle has not only been with drugs themselves, but with the repeated temptation to seek a quick pharmacological fix for a deep social and medical problem.
The Invention of the Hypodermic Syringe and Its Impact
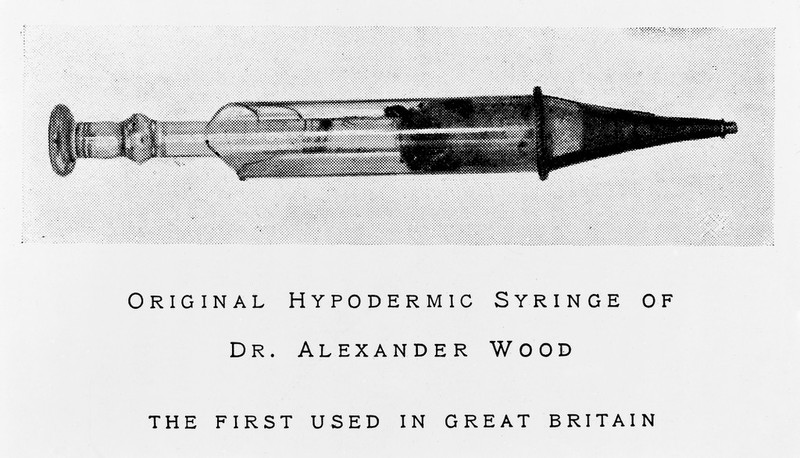
Before morphine dependence became widespread among Civil War veterans, a critical technological development had already taken place: the invention of the hypodermic syringe in the mid-nineteenth century. Developed to improve the precision and effectiveness of medical treatment, the syringe allowed physicians to deliver drugs directly into the bloodstream, producing faster and more predictable results than oral administration.
This innovation was driven by the need for more effective pain management and dosing control during a period of rapid medical advancement. However, the same characteristic that made the syringe valuable—its ability to deliver immediate and potent relief—also intensified the pharmacological effects of substances such as morphine. By accelerating the onset and increasing the potency, the syringe significantly increased the addictive potential of opioid medications.
When morphine was introduced extensively during the Civil War, it was not simply the drug itself that contributed to widespread dependence, but the combination of the drug and the method of delivery. The syringe transformed morphine from a powerful medicine into a substance with far greater capacity for dependency, setting the stage for the first large-scale opioid crisis in the United States.
Why Civil War Veterans Became Addicted to Morphine
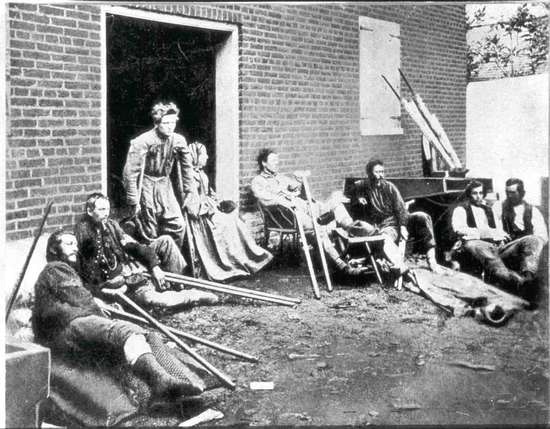
Civil War veterans became addicted to morphine for reasons that were tragically practical. Nineteenth-century military medicine had very few effective tools for severe pain. Surgeons and army physicians used morphine and opium to treat gunshot wounds, amputations, surgical pain, internal injuries, dysentery, diarrhea, cough, and the lingering illnesses that spread through army camps (Virginia Museum of History & Culture, n.d.). The hypodermic syringe made morphine even more attractive because injected doses worked quickly and reliably. In the middle of mass casualty warfare, that speed mattered.
Many veterans also left the war with lifelong pain. Morphine was not simply used at the moment of injury; it often continued after discharge to manage chronic suffering. As a result, dependence did not develop only on the battlefield. It frequently deepened in the years after the war, when veterans tried to cope with damaged bodies, insomnia, grief, disability, and the social and economic dislocation of postwar life. Jones (2020) shows that opiate use among veterans was tied not only to acute medical treatment but also to the long aftermath of war. In that sense, Civil War opioid dependence was both a medical and a social outcome.
Equally important, addiction among veterans emerged in a period that did not yet have a modern framework for substance use disorder. Veterans who became dependent were often stigmatized as weak, immoral, or lacking self-control rather than recognized as suffering from a chronic condition. The Virginia Museum of History & Culture notes that many veterans found little sympathy and often faced shame instead of care (Virginia Museum of History & Culture, n.d.). The result was a cruel paradox: medicines that were indispensable in war created suffering that the postwar culture was poorly prepared to understand or treat.
From Morphine Dependence to the Search for a “Safer” Alternative
By the late nineteenth century, the consequences of widespread morphine use had become increasingly visible. Physicians and the public began to recognize that a medication originally intended to relieve suffering had, in many cases, created a new form of dependency. This growing awareness created both a medical and commercial incentive to identify alternatives that could provide similar therapeutic benefits without the same addictive potential.
Pharmaceutical companies, operating within an environment of limited regulation and expanding consumer markets, were positioned to respond to this demand. The search for a “safer” opioid was not only a clinical endeavor but also a commercial opportunity. It was within this context that a new compound—diacetylmorphine—was introduced and marketed under the name heroin.
Why Bayer Marketed Heroin as an Alternative to Morphine
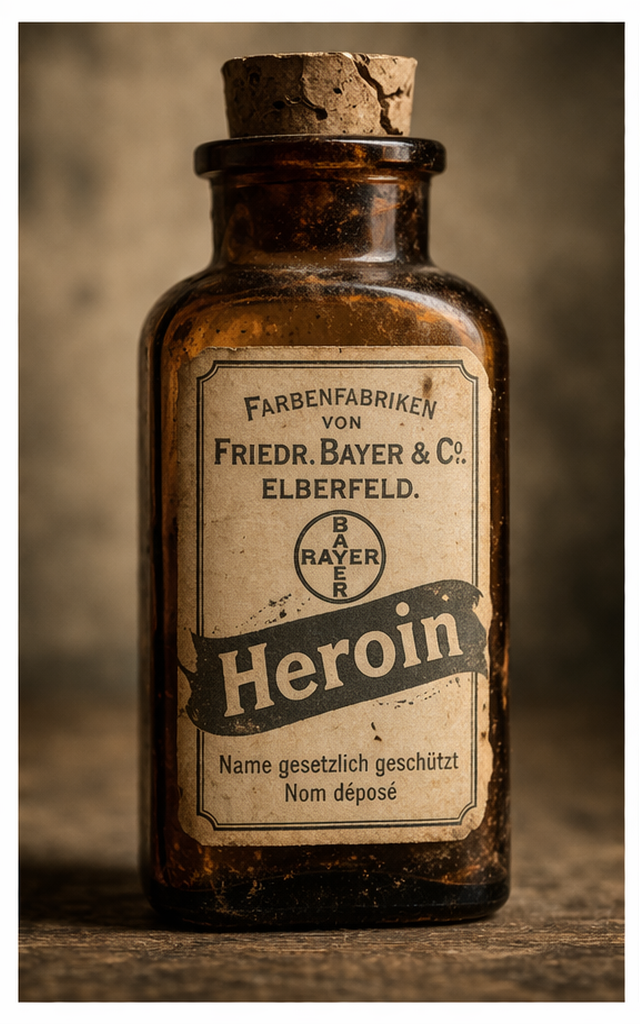
Heroin entered this landscape as another promised solution. In 1898, Bayer introduced heroin as a pain reliever and cough suppressant and presented it as a more effective and safer substitute for morphine (DEA Museum, n.d.-a; DEA Museum, 2025). That claim reflected a broader pharmaceutical logic of the era: if morphine caused dependency, perhaps a modified opioid could preserve therapeutic benefit while avoiding addiction.
That hope proved mistaken. Federal drug education materials now summarize the historical irony directly: heroin was sold as a more powerful yet supposedly less addictive substitute for morphine, but physicians soon observed escalating dependence and increasing dosage demands among patients (Drug Enforcement Administration, n.d.). Rather than solving morphine addiction, heroin created a new and often more intense problem. In retrospect, this episode stands as one of the clearest examples in American drug history of a commercialized “cure” that deepened the very crisis it claimed to address.
The heroin episode matters for more than historical curiosity. It established a pattern that continues to shape public distrust. When people today hear that a medication derived from, related to, or acting on the same receptor systems as an addictive drug is being used to treat addiction, they often remember—whether explicitly or intuitively—that the nation has heard similar promises before. The lesson of heroin is not that all medication-based treatment is fraudulent. Rather, the lesson is that pharmacologic claims require scientific scrutiny, ethical marketing, and humility.
The Harrison Narcotics Tax Act: What It Did and Why It Was Enacted
The Harrison Narcotics Tax Act of 1914 marked a major turning point in federal drug policy. Formally, it was a tax and registration law. It required manufacturers, sellers, and distributors of narcotics to register with the federal government and pay taxes, making it the first comprehensive federal law to regulate whole classes of drugs (DEA Museum, n.d.-b). It also made access to opium more difficult outside a prescription relationship with a registered medical professional (DEA Museum, n.d.-b).
The Harrison Act was enacted for several overlapping reasons. First, Progressive Era reformers had become increasingly concerned about unregulated patent medicines and narcotics markets. Second, international opium conferences had generated pressure for stronger drug controls, especially regarding opium trade and nonmedical use (DEA Museum, n.d.-b). Third, as Courtwright (1992) explains, the federal government was moving away from a largely private, medical, or local approach to narcotics and toward a more centralized system in which nonmedical narcotic use would increasingly be criminalized.
In practice, the Harrison Act did more than regulate commerce. Through later enforcement decisions and court interpretations, it narrowed the space for physicians to maintain addicted patients on narcotics and helped shift addiction from a medical problem toward a criminal one (Courtwright, 1992). That change had enormous consequences. It helped create the modern divide between legal medicine and illicit street supply, and it contributed to a policy environment in which punishment often displaced treatment. In other words, the Harrison Act was not merely enacted to organize a market. It was part of a broader political decision about what addiction meant and who would control the response to it.
Why Methadone Was Introduced to Curb Heroin Addiction
Methadone entered addiction treatment in a very different historical context. By the mid-twentieth century, heroin dependence had become a major urban public health issue, and purely punitive approaches were producing poor results. Methadone, a long-acting opioid, was shown in the mid-1960s to be effective in treating opiate addiction and was later approved by the U.S. Food and Drug Administration for that purpose (Institute of Medicine, 1995).
Unlike short-acting opioids such as heroin, methadone acts more slowly and lasts longer in the body. According to the National Institute on Drug Abuse, it reduces withdrawal symptoms and cravings while producing less intense pleasure than heroin or fentanyl (National Institute on Drug Abuse, 2025).
Methadone was introduced to curb heroin addiction because clinicians and researchers needed a treatment that could stabilize people physiologically enough for them to function, avoid withdrawal, reduce compulsive drug-seeking, and step out of the daily cycle of illegal opioid use. It was not designed as a moral cure; it was designed as a practical and medical one. The underlying logic was straightforward: if heroin dependence is driven by a chronic pattern of craving, withdrawal, and compulsive use, then a long-acting medication can interrupt that cycle more effectively than detoxification alone.
Even so, methadone inherited the suspicion generated by earlier substitution efforts. Critics argued that it merely replaced one opioid with another. Supporters argued that this criticism misunderstood the difference between chaotic, dangerous heroin use and medically supervised stabilization. Current federal sources support the latter position. NIDA states that methadone, buprenorphine, and naltrexone are effective, FDA-approved treatments that reduce overdose risk and improve outcomes, while SAMHSA emphasizes that these medications do not simply substitute one drug for another but help normalize brain chemistry and relieve cravings (National Institute on Drug Abuse, 2025; Substance Abuse and Mental Health Services Administration, 2025).
Methadone itself has a distinct origin. First developed in Germany during World War II, it was later introduced in the United States as a treatment for heroin dependence in the mid-twentieth century. Its long-acting pharmacological properties made it effective in stabilizing individuals and reducing withdrawal symptoms.
While methadone represents a more evidence-based and clinically supported intervention than earlier substitution efforts, it remains part of a broader historical pattern in which pharmacological solutions are used to address substance-related problems. This pattern raises an ongoing question within addiction policy: to what extent are these interventions resolving the underlying issue, and to what extent are they managing it within a continuing cycle of dependency and treatment?
Today’s Debate: Treatment, Substitution, and the Role of Government and Industry
This history helps explain why some people today believe that government and “big pharma” are still trying to sell drugs as the answer to drug addiction. That concern is not baseless, but it needs to be stated carefully.
On one hand, modern medications for opioid use disorder are supported by substantial evidence. NIDA reports that these medications reduce overdose deaths and other harmful outcomes, and SAMHSA identifies methadone, buprenorphine, and naltrexone as evidence-based treatments for opioid use disorder (National Institute on Drug Abuse, 2025; Substance Abuse and Mental Health Services Administration, 2025). From a clinical and public health standpoint, these medications save lives.
On the other hand, public skepticism is historically understandable because pharmaceutical marketing played a documented role in the contemporary opioid crisis. Van Zee (2009) described OxyContin’s promotion as a commercial triumph and a public health tragedy. Hadland et al. (2019) found that county-level opioid marketing to physicians was associated with increased opioid prescribing and higher opioid-related overdose mortality. CDC data underscore the magnitude of the crisis, reporting that opioid-involved deaths rose substantially from 1999 to 2023, with nearly 80,000 opioid-involved overdose deaths in 2023 alone (Centers for Disease Control and Prevention, 2025).
The most defensible critique, then, is not that all addiction medications are another version of Bayer’s heroin. That would collapse important medical distinctions and ignore strong evidence for medication treatment. The stronger critique is that the United States has repeatedly allowed market incentives, industry influence, and a narrow focus on chemical management to dominate the addiction conversation. When medications are presented as the whole answer—without housing, counseling, mutual aid, employment support, trauma care, family rebuilding, and long-term recovery infrastructure—the country risks repeating an old mistake.
The problem is not medication itself. The problem is a treatment philosophy that becomes too pharmaceutical, too commercial, or too thin to address the full human reality of addiction.
Despite the dominance of pharmacological and policy-based responses, these approaches alone have not resolved the underlying problem of addiction. As the preceding history demonstrates, each new intervention—whether chemical or regulatory—has addressed part of the issue while leaving other dimensions unresolved. This limitation created space for alternative approaches to emerge, particularly those focused on long-term behavioral change, social support, and sustained recovery outside formal medical systems.
The Emergence of the Recovery Movement
While medical and policy responses to addiction evolved throughout the twentieth century, a parallel movement emerged outside formal systems—one grounded in peer support, shared experience, and long-term behavioral change. The founding of Alcoholics Anonymous in 1935 by Bill Wilson and Dr. Robert Smith marked a significant departure from purely medical or institutional approaches. Drawing on personal experience, mutual aid, and a set of guiding spiritual principles, Alcoholics Anonymous introduced a model of recovery centered on sustained abstinence and long-term personal transformation. This approach, documented in foundational AA literature and subsequent historical accounts, demonstrated that recovery could be achieved and maintained outside of formal treatment systems (Alcoholics Anonymous World Services, 2001; Alcoholics Anonymous World Services, 1957).
By the 1950s, this movement expanded with the development of Narcotics Anonymous, which broadened the framework from alcohol-specific recovery to a more inclusive understanding of addiction. This shift—from being “powerless over alcohol” to “powerless over addiction”—reflected a more comprehensive and adaptable approach.
At the same time, Charles Dederich and the Synanon movement helped establish the therapeutic community model, emphasizing structured environments, accountability, and total lifestyle transformation. Together, these approaches formed the foundation of the modern recovery movement, demonstrating that long-term recovery could be achieved outside of traditional medical frameworks.
From Chemical Solutions to Human Solutions: Recovery, Aging, and the Next Phase
This broader recovery movement did not unfold uniformly across the United States; rather, it developed differently depending on local policy environments and social conditions. In California, where regulatory environments were comparatively permissive, Narcotics Anonymous was able to establish itself earlier and expand into other regions following its founding in 1953. This earlier development would later contribute to the presence of individuals aging in long-term recovery on the West Coast.
In New York City, however, the trajectory was markedly different. Early efforts to establish Narcotics Anonymous were unsuccessful, and the broader treatment landscape included institutional approaches such as Governor Nelson Rockefeller’s Narcotics Addiction Control Commission (NACC), which reflected an initial attempt to address addiction through treatment.
When these efforts failed to produce the desired outcomes—and as addiction increasingly affected public order, tourism, and the broader economy—political and social pressure mounted. Rockefeller, a fiscal conservative and social liberal, responded by enacting the Rockefeller drug laws in the early 1970s, among the most punitive drug policies in the nation. These laws emphasized incarceration over treatment and significantly constrained the development of community-based recovery. Their influence extended beyond New York, shaping the national policy climate that would later be reinforced under Richard Nixon’s “War on Drugs.”
As these policies were gradually relaxed in the late 1970s and early 1980s, conditions emerged that allowed for the reintroduction of Narcotics Anonymous. By 1981, NA began to take hold in a sustained and meaningful way, enabling thousands of individuals in New York City to achieve long-term recovery through a decentralized, peer-driven model.
Today, that population is aging.
The individuals who entered recovery in New York City during the late 1970s and early 1980s now represent a distinct cohort. Many are between 60 and 80 years old and have maintained continuous recovery for decades. While similar populations exist in other regions, including California, where earlier recovery communities developed, the New York City cohort reflects a unique convergence of policy history, social conditions, and the timing of Narcotics Anonymous’ reestablishment.
Despite their longevity in recovery, these individuals remain largely unrecognized within both aging services and recovery systems. Aging services are not typically designed with recovery in mind, while recovery systems have historically focused on early-stage recovery rather than long-term survivorship. As a result, this population exists at the intersection of two systems that have yet to be integrated.
A survey conducted by the author (N = 202) provides empirical evidence of this population’s presence and needs. The data indicate that the majority of respondents fall within the 60–79 age range, with 59.1% between 60–69 and 29.8% between 70–79. In terms of recovery duration, nearly half of the respondents (49.5%) reported more than 31 years of continuous recovery, with an additional 19.5% reporting 21–30 years.
The findings also highlight emerging needs associated with aging. Approximately 39.7% of respondents indicated that they anticipate needing assistance with daily living activities such as cooking, cleaning, transportation, and accessing meetings, while an additional 20.6% were uncertain. The most commonly identified future needs included transportation to meetings or appointments (58%), assistance with household tasks (48.1%), and opportunities for social connection within the recovery community (42.5%). Additional needs included help navigating healthcare systems (29.8%) and accessing caregiving support (30.4%).
Importantly, 78.1% of respondents indicated they would use services specifically designed for individuals aging in recovery if such services were available, while only 1.5% said they would not. These findings demonstrate not only the existence of a clearly defined population but also a measurable demand for targeted services.
The emergence of individuals aging in recovery—particularly within New York City—represents both a service gap and a societal opportunity. These individuals possess decades of lived experience that can inform and strengthen recovery efforts for future generations. At the same time, supporting this population through aging-in-place models can reduce reliance on costly institutional care.
Never Alone Home Care Services (NAHCS) was developed in direct response to this need. By integrating recovery-informed care with non-medical support services, NAHCS provides a model that preserves independence, sustains dignity, and recognizes the continuing value of individuals who have maintained long-term recovery.
Conclusion
From the Civil War to the present, American addiction history shows a recurring search for a chemical answer to the harms created by earlier chemicals. Morphine eased the suffering of wounded soldiers but helped generate widespread dependence among veterans. Heroin was marketed as a safer alternative to morphine but proved more addictive. The Harrison Act sought control but helped entrench a criminalized policy model. Methadone offered a more evidence-based strategy for heroin addiction, yet it too became entangled in cultural suspicion about substitution.
The lesson for the present is neither anti-medication nor uncritically pro-medication. Rather, it is that addiction policy must be historically informed, scientifically grounded, and ethically regulated. Medications for opioid use disorder should be protected as lifesaving tools, but they should not be mistaken for a complete social response. A humane system must combine medication with recovery supports, community reintegration, poverty reduction, and vigilance against the distortions of pharmaceutical marketing. Without that broader framework, the United States will continue to oscillate between commercial promises, punitive laws, and incomplete cures.
In this sense, NAHCS represents not a departure from the historical trajectory outlined in this article, but its logical next step: a shift from repeated chemical solutions toward integrated, human-centered systems of care.
References
Alcoholics Anonymous World Services. (2001). Alcoholics Anonymous (4th ed.).
Centers for Disease Control and Prevention. (2025, June 9). Understanding the opioid overdose epidemic.
https://www.cdc.gov/overdose-prevention/about/understanding-the-opioid-overdose-epidemic.html
Courtwright, D. T. (1992). A century of American narcotic policy. In D. R. Gerstein & H. J. Harwood (Eds.), Treating drug problems: Volume 2: Commissioned papers on historical, institutional, and economic contexts of drug treatment. National Academies Press.
https://www.ncbi.nlm.nih.gov/books/NBK234755/
Drug Enforcement Administration. (n.d.). Did you know that heroin was originally used as a cough remedy?
https://www.getsmartaboutdrugs.gov/media/did-you-know-heroin-originally-used-cough-remedy
DEA Museum. (2025, January 2). Bayer heroin bottle.
https://museum.dea.gov/video-archive/stories-from-the-collection-heroin-bottle
DEA Museum. (n.d.-a). Heroin bottle.
https://museum.dea.gov/museum-collection/collection-spotlight/artifact/heroin-bottle
DEA Museum. (n.d.-b). Opium order form.
https://museum.dea.gov/museum-collection/collection-spotlight/artifact/opium-order-form
Hadland, S. E., Rivera-Aguirre, A., Marshall, B. D. L., & Cerdá, M. (2019). Association of pharmaceutical industry marketing of opioid products with mortality from opioid-related overdoses. JAMA Network Open, 2(1), e186007.
https://doi.org/10.1001/jamanetworkopen.2018.6007
Institute of Medicine, Committee on Federal Regulation of Methadone Treatment. (1995). Federal regulation of methadone treatment. National Academies Press.
https://www.ncbi.nlm.nih.gov/books/NBK232105/
Jones, J. S. (2020). Opium slavery: Civil War veterans and opiate addiction. Journal of the Civil War Era, 10(2), 185–212.
Narcotics Anonymous. (1982). Narcotics Anonymous. Narcotics Anonymous World Services.
National Institute on Drug Abuse. (2025, March 20). Medications for opioid use disorder.
https://nida.nih.gov/research-topics/medications-opioid-use-disorder
Substance Abuse and Mental Health Services Administration. (2025, August 25). Medications for substance use disorders.
https://www.samhsa.gov/substance-use/treatment/options
Van Zee, A. (2009). The promotion and marketing of OxyContin: Commercial triumph, public health tragedy. American Journal of Public Health, 99(2), 221–227.
https://doi.org/10.2105/AJPH.2007.131714
Virginia Museum of History & Culture. (n.d.). Opiate addiction in the Civil War’s aftermath.
https://virginiahistory.org/learn/opiate-addiction-civil-wars-aftermath
White, W. L. (1998). Slaying the dragon: The history of addiction treatment and recovery in America.
Yablonsky, L. (1965). The tunnel back: Synanon.
Additional Sources and Recommended Reading
Alcoholics Anonymous World Services. (1957). Twelve steps and twelve traditions.
Alcoholics Anonymous World Services. (2001). Alcoholics Anonymous (4th ed.).
Deitch, D., & Casriel, D. (1967). Synanon: The anatomy of a therapeutic community.
Janzen, R. (2001). The rise and fall of Synanon: A California utopia.
Narcotics Anonymous. (1982). Narcotics Anonymous. Narcotics Anonymous World Services.
White, W. L. (1998). Slaying the dragon: The history of addiction treatment and recovery in America.
White, W. L. (2000). Toward a new recovery movement: Historical reflections on recovery, treatment, and advocacy.
White, W. L. (2014). Recovery rising: Science and stories of hope.